Epiphora or watering from the eyes can occur when there is any blockage in the Tear drainage pathway. The watering can sometimes be sticky and purulent.
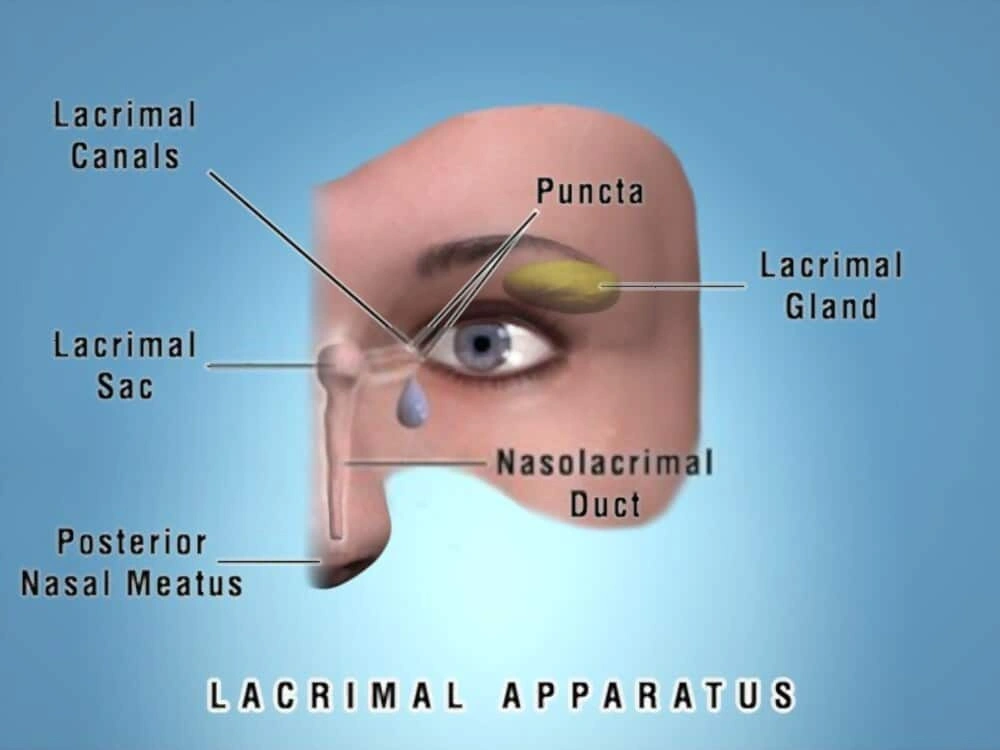
The tear drainage pathway is a network of small pipes and is called the lacrimal drainage system. The pipes start from the puncta- a small opening present in the eyelids which open into canaliculi leading to the lacrimal sac, finally ending as the nasolacrimal duct within the nose.
Many conditions can affect this pathway leading to watering from the eyes at any age group- babies to adults.

Conditions affecting the proximal drainage system i.e. puncta and canaliculi include inflammations, infections and blockages-
A thorough clinical evaluation by a trained Oculoplasty specialist and adequate management is necessary in the form of eyedrops or sometimes surgical procedures.
This condition is the narrowing of the small openings present at the eyelids. Punctoplasty is a procedure performed to restore patency
This is a condition in which inflammation causes narrowing of the tear drainage pathway. It can affect the puncta and the canaliculi. Treatment involves eyedrops to control the inflammation and sometimes inserting a stent to salvage the canaliculus and punctum.
Any injury or trauma to the area around the eye may sometimes result is laceration or cuts of the eyelids. Sometimes these injuries may also result in laceration of the small tear ducts i.e the canaliculi. It is extremely essential for its identification and early repair by a trained Oculoplastic surgeon. During the surgical repair, fine silicon tubes are placed to reconstruct and repair the canaliculi along with the eyelid laceration. This ensures there is minimal or no watering after the healing period. The surgery is performed under the operative microscope.
The sooner the surgery is performed after injury, the better are the outcomes.
“Stenosis” means abnormal narrowing or constriction of a pathway. Stenosis of the proximal drainage pathway i.e. the canaliculi can cause watering. Complete blockage of the pathway can also occur. Based on the location of the stenosis or blockage, patency can be re-established by placing a special tube called a silicon stent in the pathway. The stent is usually placed for 4 to 6 weeks and then removed.
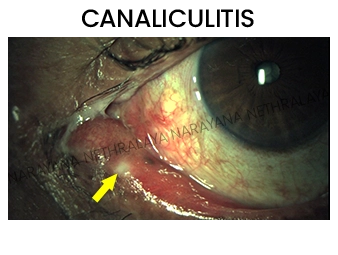
This is an infectious condition affecting the canaliculi. Patients often complain of redness and persistent sticky discharge from the eye. Evaluation by the Oculoplasty specialist includes a thorough clinical evaluation and a microbiological examination to establish the causative microbe. Initial treatment is with adequate antibiotic drops. Some cases may require an additional procedure called “Canalicular dilatation with curettage or canaliculotomy with curettage” which involves surgical removal of the pent-up pus from the canaliculus.
The nasolacrimal duct obstruction can lead to continuous watering, sticky discharge. In some cases, it can also cause a condition – Acute dacryocystitis- wherein there is intense swelling, pain and redness around the eye. The obstruction can also lead to lacrimal abscess i.e pus collection, lacrimal fistula i.e abnormal connection between the lacrimal sac and the skin causing pus discharge from overlying skin.
Though the acute inflammation can be treated by initially antibiotics, the nasolacrimal duct obstruction needs a surgical treatment i.e DCR or Dacryocystorhinostomy. In this procedure, a new alternative pathway is created between the sac and the nose. If cataract surgery is being planned, the nasolacrimal duct obstruction increases the risk of infection and hence the DCR should be performed before the cataract surgery.
Each eye has a fine pipe which drains the tears from the eye. This is a nasolacrimal duct (drain-pipe of the eye). If it gets blocked, the tears and stickiness come out of the eye. The eye can be red or feel irritation. The treatment is by dacryocystorhinostomy (DCR). This is a technique by which a new passage is created from the eye into the nose, and the tears can drain out.
DCR surgery can be performed in two ways:
The success rate in both the surgeries is good about 90-95% i.e. the outcomes are good in 90-95 patients out of 100 patients.
In the external approach, a small (about 1cm) cut is made on the side of the nose to access the tear sac. A piece of bone is removed between the sac and the nose, the sac is opened and stitched to the lining of the nose to create a passage for the tears to pass. A soft silicon stent is also passed through the passage during the healing period. The stent is removed in an OPD procedure 4-6 weeks after the surgery. The surgical scar is faintly visible after healing.
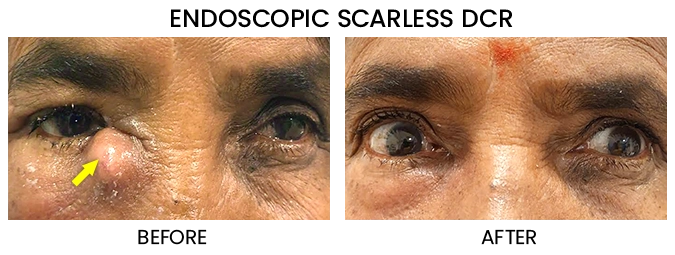
In the endoscopic approach, the entire surgery is done from within the nose. The endoscope helps the surgeon to visualize the structures from inside the nose and create a passage between the sac and the inner lining of the nose– so there is no external cut on the skin, sutures or scar. The swelling and pain soon after the surgery is usually lesser in Endoscopic DCR. In an endoscopic DCR too, a silicon stent is placed for 4-6 weeks after surgery.
A state of the art Endoscopic set up is essential- available at Narayana Nethralaya. Oculoplastic surgeons at Narayana Nethralaya trained in performing Endoscopic DCR
In some patients i.e about 5 in 100, passage may close back again due to factors such as an excessive healing response, any history of multiple attacks of infection, history of injury near the nose or prone to allergies. In these patients, the factors contributing to the closure can be assessed via an endoscope and a revision surgery can be performed. Revision DCR can be performed via external or Endoscopic approach.
Every eye has a fine pipe leading from the eye into the nose. This is like a drain-pipe, and the tears go into the throat through this pipe. This is called the nasolacrimal duct. A child may be born with a block in the naso-lacrimal duct; this condition is called congenital dacryostenosis. The water and sticky material come out of the eye, and the child’s eyes appear to the tearing all the time. This condition is seen within a few weeks after birth.
Many of the children with congenital dacryostenosis will heal only with antibiotic drops and sac massage. The oculoplastic surgeon will show you the correct technique of sac massage for your child. If the condition has not healed by 9 to 12 months, it will probably not respond to further massage and a surgery will be required.
The first step of surgery is called probing. It is very safe, can be done as a day-care procedure (night stay in hospital not required). There is no external wound or stitches, no bandage required, and normal activities can be continued from the next day.
To see a video of the procedure, play the below video. (The clipping is of a surgical procedure, viewer discretion is advised.)
Dacryocystectomy is a smaller duration surgery compared to the DCR performed for nasolacrimal duct obstruction. In this the tear sac or the lacrimal sac is removed permanently. No new passage is created to aid in tear drainage. So, watering does persist even after surgery, but there is almost no risk of infection due to the watering. The excised lacrimal sac is sent for a histopathological evaluation.
This surgery is performed only in select scenarios like an aged patient awaiting cataract surgery, patient with many health comorbidities, cases with clinical suspicion of cancer of the lacrimal sac. The surgery is performed via a small cut on the skin near the nose.
The nasal end of the tear duct or lacrimal drainage is closed during the development of the baby in the womb. At the time of birth or soon after birth, the nasal end should ideally open. In some babies, this fails to happen and they have watering and sticky discharge from their eyes from few weeks after birth. This may affect one eye or both eyes.
This condition can be initially treated with “Lacrimal sac compressions”. Lacrimal sac compression is a type of massage performed- the correct technique is important and demonstrated by the Oculoplastic specialist. This is performed till the child is about 12-18 months old. If the watering persists even after the lacrimal sac compressions, a procedure called “Syringing and Probing” is performed.
Syringing and probing is a very safe day care procedure i.e there is no overnight hospital stay. In this procedure, the obstruction is overcome surgically with a wire like instrument called lacrimal probe. The success rate increases when performed under visualization with an Endoscope. Endoscope is a camera which helps the surgeon see the nasal cavity and its structures. There is no external scar, wound or stitches post this procedure. No bandage is required and normal activities can be continued from next day.
The best results are achieved at about one year of age. Nine out of ten babies have the problem corrected if probing is done within this time. As the child grows older, success chances decrease to about 7 or 8 out of 10.
A probing can be repeated 3 months later, putting silicone intubation in to prop open the nasolacrimal duct. For children older than 3-4 years, we recommend using silicone intubation routinely at the time of probing. If this too does not resolve the watering, the next step is a bigger surgery (DCR) where a new nasolacrimal duct is constructed. But do not worry, the vast majority of children will recover only with probing.
When a nasolacrimal duct is blocked, the dirt and discharge accumulate in the lacrimal sac next to the eye. There is the risk of severe eye infection if the condition is left untreated. There may be swelling, pain, and watering. If a cataract surgery is planned, a blocked nasolacrimal duct increases the risk of dangerous infection; a DCR should be done before the cataract surgery.
DCR can be performed in two ways- externally, through a small (less than half inch) line next to the nose; endo-nasally- through the nose.
The external DCR leaves a fine mark near the eye; it has the highest success rates, more than 95 out of 100 patients have the problem completely solved after external DCR. An endo-nasal DCR is done through the nose, so there is no mark outside. The success rates are a little lower; the space inside the nose is not suitable in all patients for endonasal surgery. However, it works well in properly selected patients. Trans-canalicular Laser DCR is a very rapid procedure, with hardly any pain and swelling. However, some of the DCR done with laser may close down again.
As mentioned, about 5 out of 100 patients find that their DCR has closed down again. This may particularly happen in a patient who had multiple attacks of infection earlier, with a history of injury near the nose, or a patient who has frequent nasal allergies and colds. The DCR can be repeated, with addition of silicone intubation to prop the passage open. A typical oculoplastic surgeon will often see patients sent over from elsewhere after the DCR did not work; most such patients can be re-operated successfully
Any patient with nasolacrimal duct obstruction at any age is suitable for surgery. In some individuals with narrow nasal cavity, an additional procedure called septoplasty may be necessary to create additional space.